The Silent Killer of Enterprise CoCM: Why Epic and Spreadsheets Fail Where Mirah Wins

The Silent Killer of Enterprise CoCM: Why Epic and Spreadsheets Fail Where Mirah Wins
For a large health system, "manual" is synonymous with "unscalable." While a single clinic might manage 30 or 40 patients on an excel sheet or in their EMR, a system managing 5,000 enrolled patients across 15 primary care sites faces a mathematical impossibility.
The industry’s default assumption that Epic’s Compass Rose module is a "free" or "natural" solution is a dangerous oversight. There is a fundamental gap between a system of record (built for documentation) and a system of action (built for CoCM). When health systems choose a tool that lacks purpose-built automation, they aren't saving money on software; they are overspending on their largest line item: care manager payroll. This post explores why relying on generic EHR modules (often designed for broader case or population health management) is a recipe for operational collapse and how shifting to a "system of action" turns a cost center into a sustainable clinical engine.
1. The "Epic" Paradox: Why Compass Rose Isn’t Enough
The logic seems sound: “We already pay for Epic, so let’s just use Compass Rose.” For Collaborative Care (CoCM), however, this often creates more friction than it solves.
The Build Cost & Time Factor: Epic’s Compass Rose module doesn’t work for CoCM out of the box (we’ve spoken to many health systems across the country who have tried). There is a cost associated with building out Compass Rose and the opportunity cost of the time it takes (which we’ve seen take years).
The Workflow Friction: Compass Rose is built as a broad case-management tool, not a purpose-built CoCM engine. It requires clinicians to click through dozens of screens to find the specific clinical data (like PHQ-9 trends) that a care manager and psychiatric consultant need in seconds.
The "Registry" that Doesn't Act: In Epic, the "registry" is often just a static list. It lacks the sophistication to prioritize caseloads based on clinical response, alert staff to patients requiring urgent intervention, or provide the proactive "nudges" care managers need to optimize their time.
The Billing Nightmare: The CoCM codes are time-based. Epic struggles to automatically aggregate minutes from standard activities (phone calls, chart reviews, consultations) into a clean, audit-ready monthly report. This leaves staff manually "cell-matching" and tallying minutes which is the exact labor leakage that kills the ROI of CoCM.
2. The Labor Leakage: Losing Thousands of Clinical Hours
The Behavioral Health Care Manager (BHCM) is the heart of the Collaborative Care Model, but they are also its greatest expense. In a standard EHR workflow, we see a phenomenon called "Administrative Creep," where up to 40% of a BHCM’s week is consumed by data navigation rather than patient intervention.
When a BHCM spends their morning "cell-matching" spreadsheets or clicking through 15 tabs in Epic to find a PHQ-9 trend, that is Labor Leakage. It’s not just a productivity hit; it’s a direct drain on the program's ROI. If your technology forces a BHCM to cap their caseload at 50 patients because the "paperwork" is too heavy, you are paying 100% of a salary for 50% of the potential clinical output.
The Mirah Solution: A Centralized Command Center
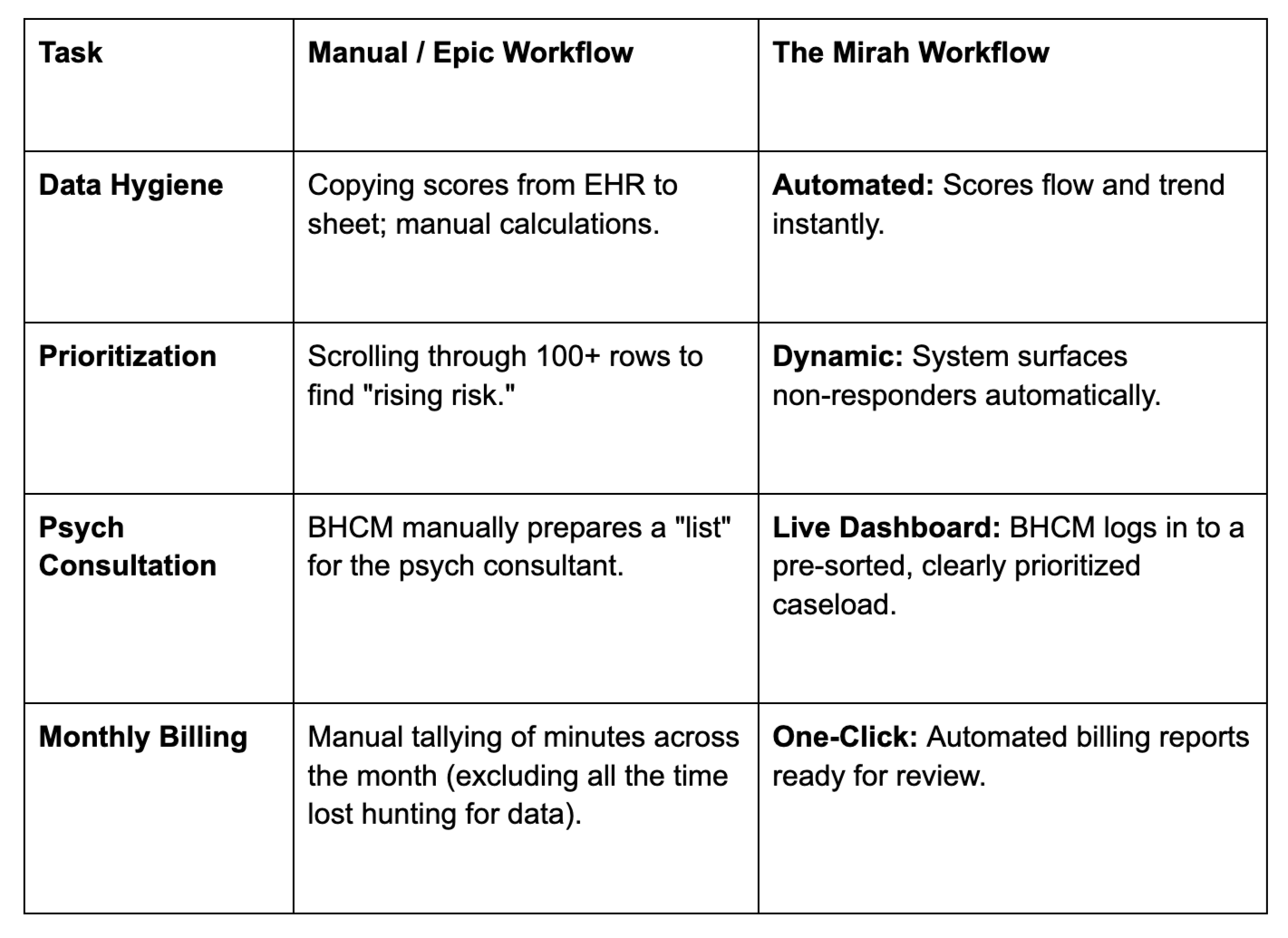
Mirah replaces the "Spreadsheet of Doom" and the clunky EHR workaround with a purpose-built digital registry that acts as the nervous system of your CoCM program.
Algorithmic Prioritization: Instead of a BHCM hunting for patients, Mirah automatically flags those whose scores haven't dropped by 50% in 60 days.
Practicing at Top of License: By automating the flags, the tracking, and the billing prep, we allow your staff to focus on therapy and consultation, not data entry.
Enterprise Scalability: Mirah provides a "bird's eye view" for leadership, allowing you to compare performance and outcomes across 15+ sites simultaneously.
The Bottom Line: If your health system is serious about population health, you cannot manage it on a tool built for accounting (Excel) or a tool built for documentation and population health management (Epic). To scale, you need a registry that works as hard as your clinicians do.
3. The Visibility Gap: The Black Box vs. Enterprise Oversight
Spreadsheets and non-purpose built EMR modules are where data goes to die. Spreadsheets and Compass Rose make it difficult for leadership to measure where and when BHCMs are actually spending their time (even more so since everything is tracked manually). Especially in VBC environments, this is a nightmare. In order to further reduce the total cost of care, it’s critical to understand who did what, at what time, and how long it actually took. No more guessing, which creates significant audit risk and potential revenue clawbacks during a CMS review.
The Blind Executive: For health system leadership, relying on Compass Rose or spreadsheets creates a dangerous transparency gap. You cannot manage what you cannot measure, and generic EHR modules often function as a "black box" where data is entered but insights rarely emerge. Without a tool designed to surface real-time KPIs, program success is left to guesswork. Instead of identifying rising-risk patients proactively, leaders are forced into a reactive stance, only seeing "high-utilizers" or poor remission rates after a patient has already hit the Emergency Department.
The VBC Loss: In a Value-Based Care environment, "guessing" is a liability. Spreadsheets and non-purpose-built EHR modules like Compass Rose are where granular data goes to die. Because these tools lack automated time-tracking and sophisticated reporting, leadership is left blind to how BHCMs are actually distributing their effort.
4. The Elephant in the Billing Room: The Care Manager Cost
When evaluating CoCM solutions, it’s easy to get distracted by "free" or low-cost platform offers. We need, however, to be honest about the math: The single biggest cost of a CoCM implementation isn't the software, it’s the Care Manager.
A dedicated care manager is the engine of the model, but they are also a significant line item expense. If your technology partner doesn't provide the efficiency required to scale, you’re left holding the bill.
Why "Free" Can Be Expensive
With a platform like Compass Rose, the value proposition hinges on more than just access; it hinges on throughput.
The Breakeven Point: If your care manager’s caseload is bogged down by manual tracking or clunky workflows, you won’t bill enough to cover their salary.
The Sustainability Gap: If you can’t bill more than the literal cost of the human being providing the care, there is nothing "free" about the implementation. It’s a net loss.
To make CoCM work, your care manager needs to be empowered to manage a high-volume registry with surgical precision. Without that efficiency, "free" software is just an expensive way to lose money on payroll.
Conclusion: Efficiency is the Only ROI
At the end of the day, CoCM is a volume-based clinical model. To provide life-changing behavioral health integration without draining your clinic's resources, you need a partner that understands the bottom line.
We don't just provide a place to track patients; we provide the clinical architecture to ensure your Care Manager is an asset, not a liability. Because if the billing doesn't outpace the paycheck, the model fails and so do the patients who rely on it.